
Essential Healthcare for Everyone, As in All Other Industrialized Nations

The Challenge:
The health care system in the U.S. is excessively expensive, ineffective, and unjust. We are spending far too much, our medical outcomes are mediocre, and we are the only nation in the industrialized world that fails to provide millions of people with basic health care.
While the U.S. spends more than twice per capita than the average spent by all nations throughout the industrialized world for medical care, it obtains far worse results than most, and is alone in failing to provide essential health care to all of its citizens.
About 45,000 Americans die each year because they don’t have health care insurance coverage.[1] That doesn’t happen in any other industrialized nation.[2]
Around 700,000 Americans go bankrupt each year because of medical bills.[3] That doesn’t happen in other developed countries.
There is significant racial inequality in the provision of health care in the United States. “Blacks and Hispanics are less likely than whites to get treatment for serious disease and more likely to die from the illness. A universal health care network, like those in place in Europe and East Asia, would eliminate this basic inequality in American life.”[4]
All the other developed countries on earth have made a different moral decision. All the other countries like us – that is, wealthy, technologically advanced, industrialized democracies – guarantee medical care to anyone who gets sick. Countries that are just as committed as we are to equal opportunity, individual liberty, and the free market have concluded that everybody has a right to health care – and they provide it. One result is that most rich countries have better national health statistics – longer life expectancy, lower infant mortality, better recovery rates from major diseases – than the United States does. Yet all the other rich countries spend far less on health care than the United States does.[5]
The bizarre and unique inequity in the U.S. health care system is vividly portrayed in the case of Canadian skier Sarah Burke, who died nine days after a training accident at Park City Mountain Resort in Utah during January 2012. At the time of her death, her medical bills had reached about $200,000. Her family would have faced bankruptcy had Sarah not been the iconic face of freeskiing. Fortunately for Sarah’s family, her fans stepped forward and donated enough money to pay off her medical bills.
“The irony is that had the accident occurred in Canada . . . her care would have been covered because, unlike the U.S., Canada has a system of universal coverage,” wrote Wendell Potter, an insurance executive-turned-whistleblower . . . “No one in Canada finds themselves in that predicament, nor do they face losing their homes as many Americans do when they become critically ill or suffer an injury . . . “ [6]
In other developed nations, there are inherent incentives, not present in the U.S. system, to provide preventive care. Medical providers are paid to keep people healthy, not just to provide tests for and procedures on sick people. In the fee-for-service system in the U.S., doctors are paid only for exams, tests, and procedures on sick people – not for keeping them well.
In other industrialized nations, the payments from insurance premiums that do not go toward health care are a small fraction of such costs in the U.S., where approximately 20% of all insurance premiums go toward the costs of marketing, underwriting, compensation for executives and salespeople, paperwork, and dividends for investors.
On average, people in other industrialized nations access their doctors more frequently than in the U.S. and their medical outcomes are far superior. “Among nineteen wealthy countries, the United States ranked nineteenth in curing people who could be cured with decent care. . . . The number of people under seventy-five who die from curable illness was almost twice as high in the United States as in the countries that do the best on this measure: France, Japan, and Spain.”[7] “A Commonwealth Fund study of nine developed countries between 2001 and 2004 showed that . . . Americans with diabetes die younger than diabetics in any of the other countries. After kidney transplants, Americans have the worst survival rate. . . . Among those nine rich nations, the per-capita rate of ‘Deaths Due to Surgical or Medical Mishaps’ was the highest by far in the U.S.A.”[8]
When it comes to keeping newborns alive, the United States ranks last of twenty-three wealthy countries. The U.S. rate of infant mortality is more than twice as high as in Sweden and Japan.[9] “A key reason . . . is that other rich countries offer free prenatal and neonatal care for every mother and every baby.”[10]
The U.S. per capita cost for health care is $7,400. Japan’s per capita cost is $3,400.[11] Patients in the U.S. average 5 visits to their doctors per year; Japanese patients average 14.5 visits per year. An MRI of the head costs about $1,000-$1,400 in the U.S.; in Japan it costs $105. Doctors and clinics in Japan spend about $150,000 for an MRI scanner; in the U.S., MRI scanners cost about $1.5 million.
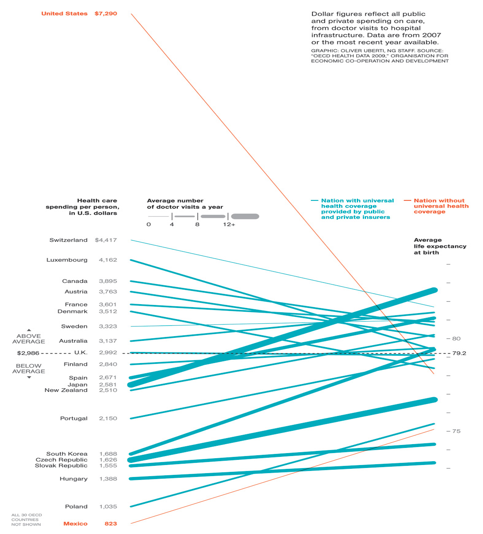
The chart below, which appeared in National Geographic (January 2010), illustrates how incredibly costly, inefficient, and tragic the U.S. health care fee-for-services, for-profit insurance-based health care system is, compared with the rest of the industrialized world (note that the cost per capita column on the left is not to scale because the U.S. cost figure would be off the top of the page):
The Record of the Democratic and Republican Parties:
Theodore Roosevelt, Woodrow Wilson, Harry Truman, Richard Nixon, Bill Clinton, and Barack Obama all advocated a major health care reform plan. However, both parties have caved to the corrupt influence of hundreds of millions of dollars spent by the medical insurance and pharmaceutical industries, depriving the American people of the coverage-for-all system heavily favored by them – and effectively leading to the many thousands of deaths and unnecessary suffering resulting from the absence of essential health care coverage common throughout the rest of the developed world.
Congress and the Obama administration worked out an unconscionable compromise health care bill that
- perpetuates the perverse stranglehold for-profit insurance companies have on our system;
- maintains the United States’s status as having the most expensive, inefficient health care system in the world; and
- will still leave 23 million people without any basic health care coverage.
How did that happen? Basically, through bribery and the worst of Washington, D.C. politics-as-usual.
During three months – April, May, and June, 2009 – the lobby blitz by insurance companies and pharmaceutical companies makes it clear how the U.S. public was shafted – and the insurance and pharmaceutical companies, once again, made a killing. During those three months, the Blue Cross and Blue Shield Association spent $2.8 million on lobbyists; GlaxoSmithKline, $2.3 million; Novartis, $1.8 million; Metlife Group, $1.7 million; Allstate, $1.5 million; Johnson & Johnson, $1.6 million; America’s Health Insurance Plans, $2 million; and Bayer Corp., $2 million. The American Medical Association spent $8.2 million on lobbying from January through June.
The second quarter of 2009 was expected to set a record, exceeding the first quarter, when health-care firms and their lobbyists spent at the rate of $1.4 million per day to prevent the health care system desired by a majority of Americans.[12]
That’s just for lobbying. The most blatant bribery comes in the form of campaign contributions. Senator Max Baucus, a Democrat from Montana, played a powerful role in the health care “reform” negotiations and was Chair of the Senate Finance Committee. He was one of the insurance industry’s hired guns, working against the public’s desire for a competing public insurance option. Here’s how the situation was described by The Guardian:
A primary target of criticism is Senator Max Baucus, the single largest recipient of health industry political donations and chairman of the finance committee that drafted the legislation criticised by [Dr. Steffie] Woolhander professor of medicine at Harvard University and co-founder of Physicians for a National Health Program].
The committee this week twice voted against including public insurance in the legislation, with Baucus opposing it both times.
Baucus took $1.5m from the health sector for his political fund in the past year. Other members of the committee have received hundreds of thousands of dollars. . . .
Baucus holds dinners for health industry executives at which they pay thousdands of dollars each to be at the table, and an annual fly-fishing and golfing weekend in his home state of Montana that lobbyists pay handsomely to attend.[13]
One lobbyist was candid about how members of Congress are bought off:
“It would be very naïve to say they’re not influenced [by campaign contributions]. The contributors certainly hope they’re influencing and the recipients probably ultimately are influenced,” he [John Jonas, of lobbying firm Patton Boggs] said. “I think it’s a morally suspect practice, and then you have to look at its application to see if it’s morally bankrupt. . . .I think what’s bad about the system is it’s got more and more lax over time.
“When I started in this practice you did not talk issues at a fundraiser. It was impolite. And then with this need for money, the system has got coarser over time so that they go around the room asking what issues you’re interested in, much more of a linkage of dollars to a discussion of the issues now.”[14]
Then there’s the revolving door, from industry, to Congress, and back to make the big bucks in industry:
At Baucus’s side, drafting much of the wording of the reform, was Liz Fowler, a senate committee counsel whose last position was vice-president of the country’s largest health insurer, Wellpoint, which stands to be a principal beneficiary of the new law.
Health companies and their lobby firms also recruit heavily among congressional staffers as a means of maintaining influence.[15]
The CBS News/New York Times Poll for July 24-28, 2009, reflected that 66% of Americans supported a government health plan option like Medicare to compete with private health insurers, with only 27% opposing that option. The poll also reflected that 55% of Americans thought the government should guarantee health coverage for all Americans, compared with only 38% who thought that is not the government’s responsibility. After many millions of dollars flowed into campaign coffers, and many more millions of dollars were spent on an intensive lobbying blitz, the desire of the public for major reform was disregarded by the White House and Congress in favor of the rapacious insurance and pharmaceutical industries.
Rocky Anderson’s Approach Toward Solutions
We must end the bizarre reliance in the United States on for-profit insurance companies for essential health care. We should adopt a health care system like Taiwan’s single-payer system (the most efficient in the world)[16] or Canada’s single-payer system (which is consistently Canada’s most popular social program).[17]
Another option might be a system like France’s (#1 in the world, according to the World Health Organization)[18], but it’s multi-payer non-profit system would likely be more expensive and less efficient in the U.S., particularly in light of the immense difficulty in the U.S. of achieving the sort of regulations that serve the public interest rather than corporate (even so-called “non-profit”) interests.
The United States should no longer be the only country in the developed world that has a grossly unequal health care system – a system that condemns millions of people to unnecessary illness and death solely because they don’t have enough money. The provision of essential health care, including preventive care, should never be dependent on how much money a person has. This is not simply a political issue; it is fundamantally a moral issue.
No child in this nation should ever suffer from a serious illness without having access to a doctor. No American woman should ever die because she could not afford a mammogram to obtain an early diagnosis of breast cancer. No man in the U.S. should die from colon cancer because he was too poor to afford a colonoscopy. No one should ever go bankrupt because of medical bills. Those horrors are now unique to the U.S. They don’t happen to people in other developed nations. We should no longer allow them to occur in the United States.
The rest of the developed world provides health care for everyone, at a far lower cost. So too can the United States – with leadership that is not bought and paid for by the insurance and pharmaceutical industries. It is simply a matter of the people of this nation rising together and saying “We won’t stand for it any more.” With strong, principled leaders, we can bring about a just, less expensive, more efficient health care system that provides better medical outcomes for the American people.
Rocky will take on major health care reform as a major priority, vigorously making the case to the public and to Congress regarding the need for a health care system that is far less expensive, more efficient, productive of better outcomes, and focused on keeping people healthy. A single-payer system, as in Taiwan or Canada, would be an enormous improvement over the costly, inefficient, unjust system perpetuated by the rapacious for-profit insurance and pharmaceutical industries.
There are many high-quality systems of health care the United States can replicate – all far superior to our absurdly expensive, inefficient, tragic system. The United States should learn from the very best among other nations, then take decisive action. The best of the following systems can be accomplished in the U.S. with a President who will fight tenaciously for what’s right.
- Single-payer National Health Insurance systems provide excellent, timely basic health care, in a manner very similar to Medicare in the U.S. In those systems, the medical providers are private, but the bills are paid by one government-run insurance program toward which every citizen contributes. Those systems are far less expensive and more efficient because there is relatively little paperwork; there is no need for marketing; there are no underwriting personnel whose jobs are to deny claims; and there is no profit for shareholders. The single payer insurance program has the market power to negotiate for lower prices. (That’s why Americans travel to Canada to buy drugs that are less expensive than the identical products in the U.S.) Examples of National Health Insurance programs are found in Canada, Australia, Taiwan and South Korea. (In 2005, health expenditures in Canada were 10.1% of GDP; in Taiwan, 6.2%; and in the U.S., 16.5%.[19])
- Multiple-payer systems utilize non-profit insurance companies providing mandated minimum levels of care for everyone, without exclusions for preexisting conditions. Both providers and payers are private. These systems are found in Germany, Japan, Belgium, Switzerland, and, in different variations, France (rated as the #1 health care system by the World Health Organization) and Latin America. (As of 2005, health expenditures in Germany were 10.4% of GDP; in Japan, 8.1%; in Switzerland, 10.8%, and, again, in the U.S., 16.5%.[20])
- In National Health Service systems – known as the Beveridge Model – health care is provided and financed by the government, through tax payments. Many (but not necessarily all) hospitals and clinics are owned by the government and some, but not all, doctors are government employees. There are no medical bills. Medical treatment is a public service, like the police department or public libraries. In the U.S., the Beveridge Model is used by the Department of Veterans Affairs, which utilizes one of the purest models of socialized medicine and garners consistently high ratings in surveys of patient satisfaction. Countries using the Beveridge Model include Great Britain, Italy, Spain, most of Scandinavia, and Hong Kong. These systems have low per capita costs because the government, as the sole payer, determines what doctors can do and what they can charge. Supplemental insurance can be purchased.
Rocky would provide the leadership, fighting as hard as it takes, for the implementation of a single-payer system. He would insist that, just as Taiwan did, the U.S. study the best systems throughout the developed world and incorporate what has worked the best. When William Hsiao, from Harvard School of Public Health, did that for Taiwan, he concluded that Taiwan should set up a single national health insurance system. The U.S. should do the same, without delay.
Our nation needs strong leadership. Rocky never backs down on matters of crucial principle. He will expose and work to end the corruption that has, for so many years, frustrated the will of the American people and caused hundreds of thousands of deaths and serious illness. He will foster a popular movement in which members of Congress will learn they will pay a heavy political price if they do not support a proven health care system that is less expensive, more efficient, available to everyone, and that achieves far better medical outcomes.
[1] http://articles.cnn.com/2009-09-18/health/deaths.health.insurance_1_health-insurance-david-himmelstein-debate-over-health-care?_s=PM:HEALTH Those without insurance have a 40% greater chance of death because of the lack of access to essential health care.
[2] The one exception used to be South Africa, which did not provide health care to everyone. However, even South Africa, one of the world’s most unequal societies, has committed to the phasing in of a national health care system under which everyone will be covered. “South Africa unveils universal health care scheme,” BBC News, August 12, 2011.
[3] David Himmelstein et al., “Market Watch: Illness and Injury As Contributors to Bankruptcy,” Health Affairs Web Exclusive, February 2, 2005, pp. W5-62.
[4] T.R. Reid, The Healing of America – A Global Quest for Better, Cheaper, and Fairer Health Care (Penguin Books: 2010), p. 23.
[5] T.R. Reid, supra, p. 3.
[6] Kari Huus, “Iconic skier’s death points out U.S. health gap,” http://usnews.msnbc.msn.com/_news/2012/01/30/10274212-iconic-skiers-death-points-out-us-health-gap#.Tydgpvleex4.facebook .
[7] T.R. Reid, supra, p. 32.
[8] Id.
[9] Cathy Shoen et al, “U.S. Health System Performance: A National Scorecard,” Health Affairs Web Exclusive, September 20, 2006, p. W457.
[10] T.R. Reid, supra, p. 34.
[11] T.R. Reid, supra, p. 10.
[12] Dan Eggen, “Lobbyists Spend Millions to Influence Health Care,” Washington Post, July 21, 2009.
[13] Chris McGreal, “Revealed: millions spent by lobby firms fighting Obama health reforms – Six lobbyists for every member of Congress as healthcare industry heaps cash on politicians to water down legislation,” The Guardian, October 1, 2009.
[14] Id.
[15] Id.
[16] “Taiwan built a system that uses private doctors and hospitals, with a single, government-run insurance plan to pay them. . . . The government insurance allows patients free choice of any hospital, clinic, or doctor, so providers end up competing furiously for customers. . . . The most striking result of Taiwan’s new system is a healthier population with a longer healthy life expectancy and much higher recovery rates from major diseases. . . . [E]ven with explosive growth in the consumption of medical services, national health spending in Taiwan remains at about 6 percent of gross domestic product (as opposed to about 17 percent of GDP in the United States). This has kept costs low for patients. The co-pay for a doctor visit runs about $7; the monthly premium for an entire family’s health insurance averages $150 or so. . . . Taiwan may have to pay as much as 8 percent of its GDP for its universal health care system. But even if it gets to that point, Taiwan will be at less than half the U.S. rate of health care spending – while providing coverage for everybody.” T.R. Reid, supra, pp. 172-76.
[17] “No Canadian dies because he can’t afford a doctor; no Canadian goes bankrupt from medical bills. . . . Canada has better health statistics overall than the United States, a longer healthy life expectancy, and a lower rate of infant mortality. And it achieves all that for about half the cost per capita of the U.S. system. ‘Canada’s cost advantage,’ the Canadian health care economist Robert Evans [stated], ‘is due to a much more efficient payment system and to the sheer clout that a universal system has in price negotiations.’ “ T.R. Reid, supra, p. 128.
[18] “France’s health care system . . . is not ‘socialized medicine.’ Rather, it is largely a system of private doctors treating patients who buy health insurance – from a government health plan, and from private insurers – to cover most of the cost. . . . Because the insurance plans . . . are nonprofit entities, their main concern is not providing a return to investors but, rather, paying for people’s health care. . . . French insurance funds can’t turn you down for coverage, regardless of preexisting conditions. They can’t terminate your coverage when you lose or change your job. . . . Since the French insurance funds don’t spend any money on marketing, on filtering out unwelcome customers, on reviewing and denying claims, or on paying dividends to stockholders, they are significantly more efficient businesses than American insurance companies.” T.R. Reid, supra, pp. 50-51.
[19] OECD Health at a Glance, 2009; Government of Taiwan.
[20] Id.